I understand that I have the right to revoke this authorization. I _____ do hereby request that the Thomas E.
Free 14 Release Authorization Forms In Pdf Ms Word Excel
In accordance with this request I hereby release and forever discharge and agree to hold harmless and indemnify the Commonwealth of Virginia Virginia.
Authorization for release of information. My records to the following. I authorize LifeLens Psychological And Counseling Services PLLC to release. Fill out the entire form neatly.
The letter should include the name and address of the sender state Zip code and the name and address of the recipient with the state and zip code. Authorization for Release of Information This form when completed and signed by you authorizes me to release protected information from your clinical record to the person you designate. By observing a proper authorization process the confidential information will be kept secured and will only be distributed to the people whose names are stated on the authorization form document.
Your authorization allows the Health Plan your health insurance carrier or HMO to release your protected health information to a person or organization that you choose. Authorization to Release Information Please Print This form is used to release your protected health information as required by federal and state privacy laws. You must know what is in it to write an authorization letter to disclose information.
Ad Search Faster Better Smarter Here. Authorization Letter To Release Information should include the following. MBMC 10-3343-817 050411 Page 2 of 2.
Verbal communication with clinician clinic representative. Lets say youre wife or husband has authorization for your bank account so shehe can withdraw money from it. Name Print Tech engage in the following as it relates to my records.
Cook Counseling Center of Virginia. The Federal Rules restrict any use of the information to criminally investigate or prosecute any alcohol or drug abuse patient. Complete this form as fully as possible.
Health Information Management Services UCSF Medical Center 400 Parnassus Ave Room A88 San Francisco CA 94143-0308 YOUR RIGHTS This Authorization to release health information is voluntary. If you are signing on behalf of a patient for whom you are the legal guardian or personal representative you must attach a certifi ed copy of your appointment as legal guardian or. A general Authorization for the release of medical or other information is NOT sufficient for this purpose.
Authorization to release healthcare information This form template authorizes your healthcare provider to release your private medical records to the parties you specify. Authorization For Release Of Information. Making any further disclosure of this information unless further disclosure is expressly permitted by the written consent of the person to whom it pertains or as otherwise permitted by 42 CFR Part 2.
This Authorization to release health information is voluntary. Do not send medical records to this address. Allow a minimum of 10 business days for processing.
To know what is an Authorization Letter to Release information you must first know what is an authorization letter. 1 to conduct research-related treatment 2 to obtain information in connection with. Please note that blank items on this form may cause major delays in processing your request.
I authorize my therapist andor his or her administrative and clinical staff to releaseexchange. Medical professionals financing agents employers and even faculty members need to submit a Release Authorization Form to allow themselves to access the information of a particular person. Yale New Haven Health Health Information Management Release of Information Services PO Box 9565 New Haven CT 06535.
It also includes a letter date. My childs records to the following. Treatment payment enrollment or eligibility for benefits may not be conditioned on signing this Authorization except in the following cases.
An authorization letter is a written confirmation that you approve somebody to do or to have something. Ad Search Faster Better Smarter Here. A student may grant access to these records to a designated party by completing this form.
Directions for Completing the Authorization for Release of Protected Health Information Form. Authorization for Release of Information GSA. Treatment payment enrollment or eligibility for benefits may not be conditioned on signing this Authorization.
Return completed authorization by mail fax or email as designated below. This release must be signed by the student. A general authorization for the release of medical or other information is sufficient for this purpose.
AUTHORIZATION FOR RELEASE OF INFORMATION. Return Completed Authorization To. Information is included for a patient age 13 or older the minor must sign as described above.
This authorization shall be in effect until. AUTHORIZATION FOR THE RELEASE OF INFORMATION Student Signature Date The Family Educational Rights and Privacy Act of 1974 as amended affords privacy rights to students with respect to their education records.
Record release form templates for ms word word amp excel regarding release of information form template. 10 best medical release form examples amp templates pdf within release of information form template.
Form Hipaa F 3 Download Printable Pdf Or Fill Online Authorization For Release Of Information One Way From Department Of Mental Health Massachusetts Templateroller
Printable Mental Health Release Form.
Release of information form template mental health. _____ Authorization and Signature. Ad The 1 Source For Premium Website Templates. Start Working with Your Docs.
Release of genetic testing information Health and Safety Code 124980j. Purpose of Information Release. This form template authorizes your healthcare provider to release your private medical records to the parties you specify.
It may be printed or a digital one. Mail or fax to HIM ROI sidebar. Add Signature Fields Collect eSignatures.
Information pertaining to mental health diagnosis or treatment Welfare and Institutions Code 5328 et seq Release of HIVAIDS test results Health and Safety Code 120980g. There are various form formats and you can get release of information and Talent Release Form templates all free of cost. Ad Save Time Signing Sending Documents Online.
Start a free trial now to save yourself time and money. They are utilized to gather or provide. Click here to instantly download the FREE Release of Information form.
Start Working with Your Docs. Insert Name of Person or Title of Person or Organization Description of Information to be Disclosed PatientClient should initial each item to be disclosed. 40 medical records release form release of information with regard to release of information form template.
The should fill a form occurs every now and then. This form allows you to provide consent to share information regarding 1 behavioral and mental health services and referrals and 2 treatment for alcohol or substance use disorder. 20 samples of medical records release amp authorization forms inside release.
State law requires each clients consent for the release of confidential information related to mental health or developmental. Learn how to complete an authorization form. Signing this form to release my health information to the party or parties I have designated.
Authorization to release healthcare information. Ad The 1 Source For Premium Website Templates. All mental health information including assessment diagnosis and treatment.
Authorize Insert Name of Mental Health Counseling Organization to disclose to andor obtain from. ThemeForest 45000 WP Themes Website Templates From 2. Highland Hospital Health Information Management Release of Information 1000 South Ave Box 55.
Release of Information Form. The most secure digital platform to get legally binding electronically signed documents in just a few seconds. Further mental health care Payment of insurance claim Legal investigation Applying for insurance Vocational rehab evaluation Disability determination At the request of the individual Other specify.
Mental health release of information form template Business types are used by everybody for any reason or other in both offices in addition to private payments. This template can be used to coordinate the release of confidential information during a clients transition of care or other cicrumstances where private records need to be shared. _____ the following information.
Hence the availability of important forms and formats which will facilitate your applications with employers government bodies and other organizations will always be there with the rich template resources. Get Yor Website Online Today. Add Signature Fields Collect eSignatures.
I do not have to sign this authorization and that my refusal to sign will not affect my abilities to obtain treatment from the New York State Office of Mental Health nor will it affect my eligibility for benefits. Get Yor Website Online Today. Complete this form to opt-out of the Care Everywhere Agreement.
Get Started for Free. ThemeForest 45000 WP Themes Website Templates From 2. Ad Save Time Signing Sending Documents Online.
Fill out securely sign print or email your new mexico hipaa release form mental health instantly with SignNow. Get Started for Free. One must write or enter information.
I am requesting that my Protected Health Information be disclosed for the. It may be a job form a contract sale deed agreement insurance coverage lease form bank form medical form human assets kind and so on. Free free medical records release authorization form hipaa mental health release of information form template pdf A Type is basically a record with blank spaces.
Available for PC iOS and Android. For the rest of your necessary Intake forms check out our Easy Intake Packet which includes the 7 essential counseling Intake forms you need all in one instantly downloadable Microsoft Word template. If you have any questions please contact the appropriate hospital at the number listed below.
Health information have already taken action because of my earlier authorization. A AA Unless otherwise revoked this Authorization expires _____insert. However your consent is needed to share certain types of health information.
This information will only be shared to help diagnose treat manage and.
Authorization is automatically revoked and no further disclosure of the patients information is permitted. This form is used to obtain authorization from the member to disclose their information.
Information Release Authorization Template By Business In A Box
A copy of a valid photo identification with a signature ie.
Authorize to release information form. The letter has to have the senders name and address with state and zip code as well as the recipients name and his address with state and zip code. The authorization to release information form can be used when you are going to authorize somebody to release your information to some other party. A letter date is also required.
AUTHORIZATION TO RELEASE INFORMATION Form must be notarized TO WHOM IT MAY CONCERN. Reimbursement request information including provider name substantiation and dollar amount reimbursement. What protected information will be released.
This form may also be used to request the use of a members psychotherapy notes. Authorization to Release Information. This form authorizes Via Benefits to release at your request your personal information to another person or organization that you designate.
If you choose to complete this form it must be signed by you dated and delivered to MOSERS to be effective. You must complete all information below. Please fill out copies of this form for family members you wish to have access to your medical information.
Consent to Release Information Form. Member Authorization Form To Release Information. This form may only be signed by the member whose information will be released or the.
The Authorization to Release Information form allows MOSERS to release specific information authorized by you to another person or organization. 8That unless otherwise indicated or specified here a request for disclosure or release. Authorization to release healthcare information This form template authorizes your healthcare provider to release your private medical records to the parties you specify.
A student may grant access to these records to a designated party by completing this form. Contents of Authorization Letter to Release Information To write an authorization letter to release information you need to know Its contents. 7I can have a copy of this form.
MOSERS recommends that you complete and submit this form but it is optional. IWe the undersigned hereby authorize you to release to _____ and _____ or its agents and assigns any and all information that they may require about my loan and mortgagetrust deed on the above referenced property. Authorization to Release Information This authorization form will allow Trio its authorized representatives and your designated 3rd Parties to share information about you and your co.
This form consists of three 3 pages. 6I should tell all agencies and people listed on this form when I withdraw my consent. Drivers license or identification card issued by one of the United States a US.
By observing a proper authorization process the confidential information will be kept secured and will only be distributed to the people whose names are stated on the authorization form document. Please complete the below release form to allow us to discuss your information with your designated 3rd parties. Authorization to Release Information INSTRUCTIONS.
I hereby authorize any representative of the Chief Judge of the Superior Court of the District of Columbia bearing the release or copy thereof within six months of its date to obtain any information in your files pertaining to arrest. A Release Authorization Form is a written consent of an individual to allow a third party in using and viewing his personal data and information. Medical professionals financing agents employers and even faculty members need to submit a Release Authorization Form to allow themselves to access the information of a particular person.
If you have any questions or need assistance completing this form please contact Customer Service at 800 247 -2583. Military identification card etc must be submitted with this signed form. This form when completed and signed by you authorizes us to release andor request protected health information from your clinical record to from the person you designate.
This release must be signed by the student. This authorization is a continuation. GSA3590 Authorization for Release of Information.
Personal information may include but is not limited to the following. If incomplete this authorization will be returned. Authorization to Release Information.
Authorization to Release Information This form is used to consent to the sharing of your protected health information PHI. AUTHORIZATION FOR THE RELEASE OF INFORMATION Student Signature Date The Family Educational Rights and Privacy Act of 1974 as amended affords privacy rights to students with respect to their education records. The sample form format is here and it can be used for such purposes.
This form is under legislative laws from different countries such as the FOI or Freedom of Information Act and the Information Privacy Act. Please fill out one copy of this form for each medical professional you have seen in the last two years. The completion of this form certifies that you are the memberretireebeneficiary in question and authorize TRS to release your information to the person entity or employer listed below.
I understand that if I revoke this authorization. NS HIM 0001 Rev 102912.
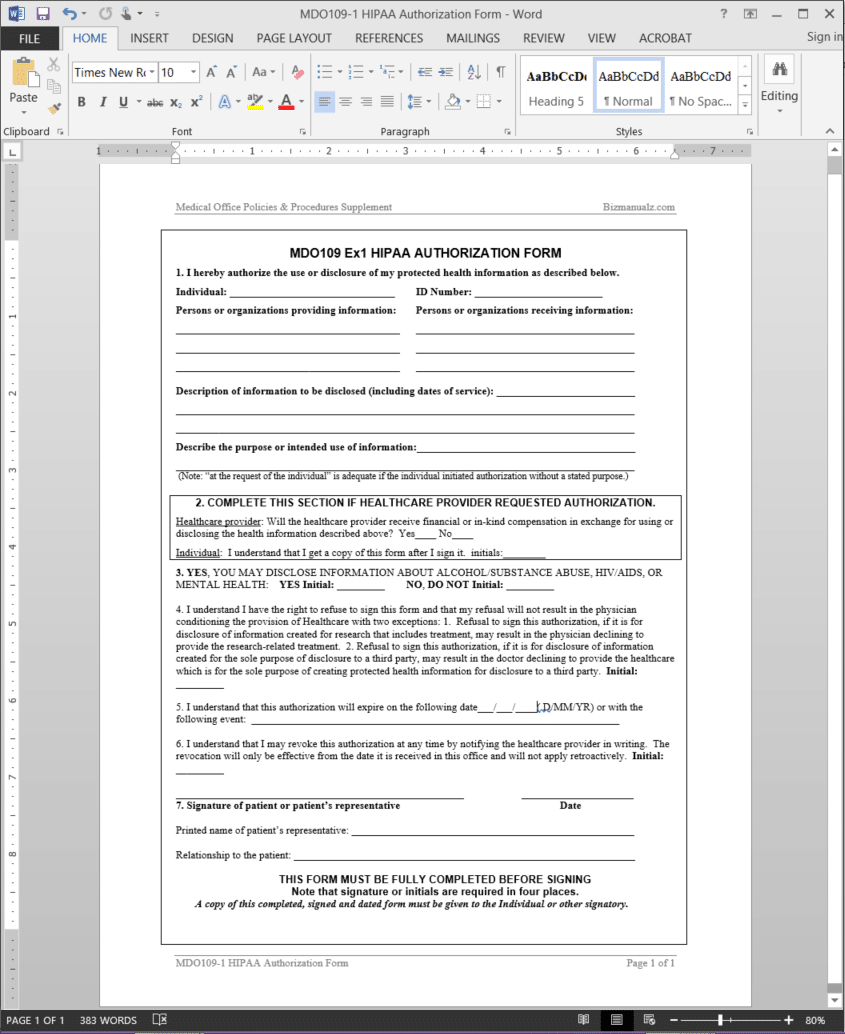
Hipaa Authorization Form Template Mdo109 1
Copy this ready-made authorization for disclosure of protected health information template to your 123FormBuilder account.

Authorization for disclosure of protected health information template. Print Name of Research Participant _____Date of Birth. Written authorization from the patient is required by law. Description Authorization Health Information Form.
Ad The 1 Source For Premium Website Templates. Sample Authorization for Disclosure of Health Information. Authorization For Disclosure Of Protected Health Information Template.
______________ I authorize the use andor disclosure of Protected Health Information Health Information. _____ SS or MRN _____ I hereby authorize UMass Memorial Medical Center a member of UMass Memorial Health Care Inc. Fill out AUTHORIZATION TO DISCLOSE PROTECTED HEALTH INFORMATION Docx in just several clicks by following the guidelines listed below.
All items must be complete to be considered valid. Fill out securely sign print or email your Authorization For Release of Protected Health Information PHI instantly with SignNow. Patient date of birth.
Forms and Handbooks Subject. 1 I hereby authorize name of provider to disclose the following information from the health records of. Name of individual_____ Release Information To_____ Purpose of.
I understand that this authorization is voluntary that the information to be disclosed is protected by law and the usedisclosure is to be made to conform to my directions. The individual also indicates the acknowledgment of his or her rights regarding consent to the use and disclosure of the information. I understand that this authorization is voluntary that the information to be disclosed is protected by law and the usedisclosure is to be made to conform to my directions.
Here you can adjust it to include more input fields or form elements. Get Yor Website Online Today. I understand I have the right to revoke this authorization at any time.
For you to authorize the disclosure of your personal information which may include health information to persons or organi-zations outside of the Division of Family Resources DFR. Mitted diseases abortion or other information I may consider sensitive. Complete all of the required boxes they are yellow-colored.
Ad The 1 Source For Premium Website Templates. Authorization and Signature I authorize the release of my confidential protected health information as described in my directions above. This form is used by an individual to consent to the use or disclosure of protected health information as described within.
Click the Get form button to open the document and move to editing. ThemeForest 45000 WP Themes Website Templates From 2. Authorization for Disclosure of Protected Health Information to Employer.
The information that is used. Your privacy is protected by state and federal privacy laws. You are trying to access a resource only available to AHIMA members.
To disclose my protected. Print Name of Patient. HIPAA AUTHORIZATION FOR USE OR DISCLOSURE OF HEALTH INFORMATION This form is for use when such authorization is required and complies with the Health Insurance Portability and Accountability Act of 1996 HIPAA Privacy Standards.
Get Yor Website Online Today. As such we need your explicit permission to make the requested disclosure. Pick the template you require from our collection of legal forms.
I authorize the release of the following information for dates of service from B. I understand this authorization will expire 90 days from the date signed unless a date is otherwise stated_____ 5. To do that you only need drag and drop efforts.
I understand that this authorization pertains to information obtained on or before the date this authorization was signed. The organization authorized to receive the information is not a health plan or health care provider the released information may no longer be protected by federal or state privacy regulations 4. Patient Name_____________________________________ Date of Birth________________.
Form 3039rn102018 Created Date. I authorize the release of my confidential protected health information as described in my directions above. Authorization to Use or Disclose Protected Health Information in Research.
Authorization to Disclosure Protected Health Information Author. The most secure digital platform to get legally binding electronically signed documents in just a few seconds. AUTHORIZATION FOR THE DISCLOSURE OF PROTECTED HEALTH INFORMATION Page 1 of 2 UMass Memorial Medical Center UMass Memorial - Community Healthlink UMass Memorial HealthAlliance-Clinton Hospital UMass Memorial - Marlborough Hospital UMass Memorial Medical Group - Location.
ThemeForest 45000 WP Themes Website Templates From 2. _____ THE PURPOSE OF THE RELEASE OF THIS INFORMATION IS FOR. Authorization for the Disclosure of Protected Health Information Name Please print.
Available for PC iOS and Android.