I understand that I have the right to revoke this authorization. I _____ do hereby request that the Thomas E.
Free 14 Release Authorization Forms In Pdf Ms Word Excel
In accordance with this request I hereby release and forever discharge and agree to hold harmless and indemnify the Commonwealth of Virginia Virginia.
Authorization for release of information. My records to the following. I authorize LifeLens Psychological And Counseling Services PLLC to release. Fill out the entire form neatly.
The letter should include the name and address of the sender state Zip code and the name and address of the recipient with the state and zip code. Authorization for Release of Information This form when completed and signed by you authorizes me to release protected information from your clinical record to the person you designate. By observing a proper authorization process the confidential information will be kept secured and will only be distributed to the people whose names are stated on the authorization form document.
Your authorization allows the Health Plan your health insurance carrier or HMO to release your protected health information to a person or organization that you choose. Authorization to Release Information Please Print This form is used to release your protected health information as required by federal and state privacy laws. You must know what is in it to write an authorization letter to disclose information.
Ad Search Faster Better Smarter Here. Authorization Letter To Release Information should include the following. MBMC 10-3343-817 050411 Page 2 of 2.
Verbal communication with clinician clinic representative. Lets say youre wife or husband has authorization for your bank account so shehe can withdraw money from it. Name Print Tech engage in the following as it relates to my records.
Cook Counseling Center of Virginia. The Federal Rules restrict any use of the information to criminally investigate or prosecute any alcohol or drug abuse patient. Complete this form as fully as possible.
Health Information Management Services UCSF Medical Center 400 Parnassus Ave Room A88 San Francisco CA 94143-0308 YOUR RIGHTS This Authorization to release health information is voluntary. If you are signing on behalf of a patient for whom you are the legal guardian or personal representative you must attach a certifi ed copy of your appointment as legal guardian or. A general Authorization for the release of medical or other information is NOT sufficient for this purpose.
Authorization to release healthcare information This form template authorizes your healthcare provider to release your private medical records to the parties you specify. Authorization For Release Of Information. Making any further disclosure of this information unless further disclosure is expressly permitted by the written consent of the person to whom it pertains or as otherwise permitted by 42 CFR Part 2.
This Authorization to release health information is voluntary. Do not send medical records to this address. Allow a minimum of 10 business days for processing.
To know what is an Authorization Letter to Release information you must first know what is an authorization letter. 1 to conduct research-related treatment 2 to obtain information in connection with. Please note that blank items on this form may cause major delays in processing your request.
I authorize my therapist andor his or her administrative and clinical staff to releaseexchange. Medical professionals financing agents employers and even faculty members need to submit a Release Authorization Form to allow themselves to access the information of a particular person. Yale New Haven Health Health Information Management Release of Information Services PO Box 9565 New Haven CT 06535.
It also includes a letter date. My childs records to the following. Treatment payment enrollment or eligibility for benefits may not be conditioned on signing this Authorization except in the following cases.
An authorization letter is a written confirmation that you approve somebody to do or to have something. Ad Search Faster Better Smarter Here. A student may grant access to these records to a designated party by completing this form.
Directions for Completing the Authorization for Release of Protected Health Information Form. Authorization for Release of Information GSA. Treatment payment enrollment or eligibility for benefits may not be conditioned on signing this Authorization.
Return completed authorization by mail fax or email as designated below. This release must be signed by the student. A general authorization for the release of medical or other information is sufficient for this purpose.
AUTHORIZATION FOR RELEASE OF INFORMATION. Return Completed Authorization To. Information is included for a patient age 13 or older the minor must sign as described above.
This authorization shall be in effect until. AUTHORIZATION FOR THE RELEASE OF INFORMATION Student Signature Date The Family Educational Rights and Privacy Act of 1974 as amended affords privacy rights to students with respect to their education records.
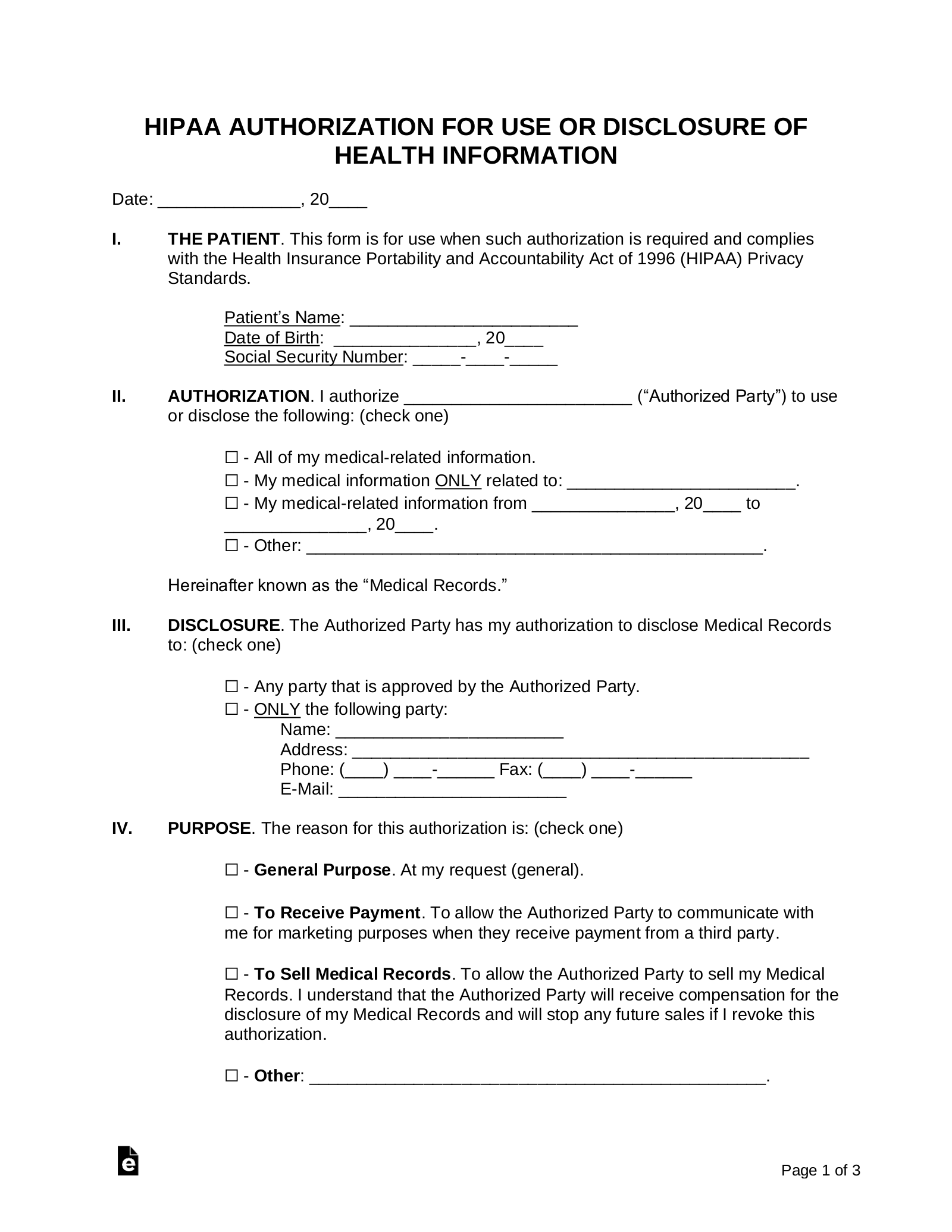
Free Medical Records Release Authorization Form Hipaa Word Pdf Eforms
Information Release Authorization Template By Business In A Box
Authorization For Release Of Information Form 2018 Western Washington Medical Group

Free Authorization To Release Information Printable Real Estate Document Power Of Attorney Form Real Estate Forms Lettering

Release Of Information Template Pdf Templates Jotform